DNP 805 How can healthcare impact the silence to violence DQ
DNP 805 How can healthcare impact the silence to violence DQ
DQ1
Discuss your results from Appendix A in Crucial Accountability
What confrontations do you typically avoid or instigate?
Do you use tricks to talk yourself out of speaking up or are
you one who always speaks?
How can healthcare impact the silence-to-violence habit?
What can you personally do?
Provide an example of a leader who does this well.
DQ2
Discuss the following about the results of your
StrengthsFinder assessment.
Do you feel it is important to surround yourself with people
who are not like you? Why or why not? What problems would you anticipate if you
did so and how would you deal with them?
What is the most valuable item you garnered from examining
your personal leadership style?
How can you use your strengths in your practice and as a
doctorally-prepared nurse?
Provide an example of a nurse leader in your experience that
has the most positive strengths.
When violence erupts in a healthcare facility, the consequences are many and unpredictable, potentially including injury or death of building occupants; property damage; lawsuits; and diminished patient, staff, and community trust. The risk of workplace violence looms in healthcare facilitieswhere a stressful work environment can quickly become volatile, visitors may be highly emotional, and drugs or expensive equipment may become targets of robbery. In addition, home care employees may walk alone into homes where patients or their family members keep weapons or dr?ugs or may visit homes in areas with high crime rates, increasing the risk of encountering violence while on the job.
Many violent events in healthcare, particularly assaults on staff members, are caused by patients; however, this guidance article focuses on violence committed by visitors, employees, and trespassers (e.g., robbery, stalking of a patient or employee, intimate partner violence). For more information on violence caused by patients, see Patient Violence.
The National Institute for Occupational Safety and Health defines workplace violence as violent acts, including physical assaults and threats of assault, directed toward personnel at work or on duty. Many other sources include verbal aggression (e.g., threats, verbal abuse, hostility, harassment) in the definition of workplace violence. Not only can verbal aggression cause significant psychological trauma and stress, it can also escalate to physical violence. (OSHA Caring)
Incidence
The Occupational Safety and Health Administration (OSHA) reports that in each year from 2011 to 2013, U.S. healthcare workers suffered 15,000 to 20,000 serious workplace-violence-related injuries; serious injuries are those that require time away from work for treatment and recovery (OSHA Caring).
Violence is significantly more common in healthcare than in other industries, such that violence-related injuries to healthcare workers account for almost as many similar injuries sustained by workers in all other industries combined. In 2013, healthcare and social assistance workers experienced 7.8 cases of serious workplace violence injuries per 10,000 full-time equivalents (FTEs), while other larges sectors such as construction, manufacturing, and retail all had fewer than two cases per 10,000 FTEs. (OSHA Caring)
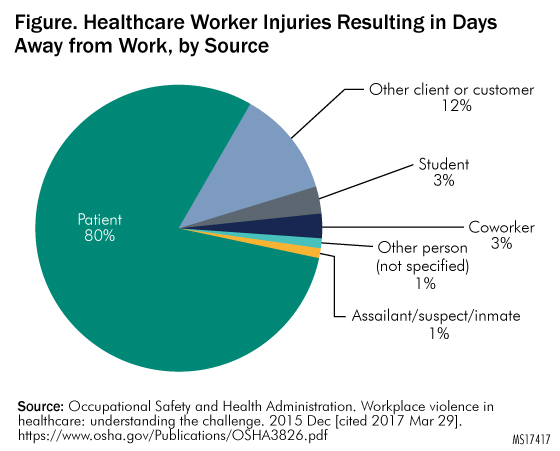
Additionally, in 2016, the U.S. Government Accountability Office (GAO) published an analysis of three federal datasets revealing that in 2013 healthcare workers at inpatient facilities such as hospitals experienced injuries from workplace violence that required time off at a rate that was five times that of overall private-sector work?ers. According to OSHA, individuals other than patients, including visitors and coworkers, cause 20% of violent incidents in healthcare. See Figure. Healthcare Worker Injuries Resulting in Days Away from Work, by Source? for an illustration.
|
?
 |
Organizational Perspective
In a violence reduction project conducted at a large American hospital that examined employee event reports involving workplace violence, an overall rate of 3.03 incidents per 100 FTEs per year was identified (Arnetz et al. Application).
Risk Factors
Healthcare workers face serious risks. As Kevin Tuohey, president-elect of the International Association for Healthcare Security and Safety, stated in a 2017 publication, While hospitals have always been looked at as places of refuge, as places that were really safe, I think in the last 10 years thats changed, and I think that they are no longer exempt. (HCPro)
The following risk factors for violence are inherent to the provision of healthcare (Joint Commission OSHA; Papa and Venella):
- Setting-specific vulnerabilities of acute care hospitals, emergency departments (EDs), community health clinics, drug treatment clinics, long-term care facilities, and private homes
- Isolated workconducted alone or in small groups, in remote areas, or in areas with high crime rates
- Late night or early morning work hours
- The economic realities of healthcare, such as reduction in staff, increased productivity pressure, patients and visitors who are experiencing difficult personal or financial circumstances
- Exchange of money with the public
- Transport and delivery of passengers, goods, or services
High-Risk Areas
Certain clinical areas are particularly vulnerable to violence perpetrated by a family member or visitor.
Emergency department. Several factors predispose the ED to violence. As the main route of public access into the facility, EDs are often understaffed and overcrowded. The American College of Emergency Physicians posits that an overall increase in violence throughout society has, in turn, increased violence in hospitals and EDs. The organization cites the following factors that increase the risk of violence in EDs (ACEP Emergency):
- Presence of gangs
- Long wait times for care, sometimes in undesirable environments
- Influence of drugs and alcohol
- Private citizens arming themselves
- Presence of individuals requiring medical clearance after an arrest by law enforcement
- Presence of individuals requiring psychiatric support in absence of sufficient dedicated mental health facilities
In one survey, more than 75% of emergency physicians reported experiencing at least one incident of workplace violence per year; nearly as many emergency nurses reported verbal or physical assault by patients or visitors. (ACEP Emergency)
In a study of ED resident physicians published in 2016, in addition to reporting varying levels of violence perpetrated by patients, subjects reported experiencing the following types and rates of violence perpetrated by visitors (Schnapp et al.):
- Verbal harassment: 86.6%
- Sexual harassment: 21.8%
- Physical violence: 11.8%
Perhaps not surprisingly, nearly a quarter of the residents surveyed reported feeling safe at work occasionally, seldom, or never. (Schnapp et al.)
Womens healthcare. Womens healthcareincluding labor and delivery and the maternal-child health unitis a high-risk environment owing to the emotionally charged issues surrounding pregnancy and childbirth. (Papa and Venella)
Intensive care unit (ICU). Because the ICU cares for the most seriously ill patients, visitors to this area may be extremely distraught, stressed, and demanding of staff attention, which mayor may appear to bein short supply. This combination can lead to verbal aggression toward staff and can escalate into physical assault, especially if staff are not properly trained in responding to distraught visitors.?
?ECRI RESOURCES
|
|---|
Neonatal or pediatric ICU. Concerned parents may become violent while waiting to talk to a physician, while waiting for test results, or after finding out that their child has an serious disease. Divorced or estranged parents may come into conflict over their childs care in nurseries or on pediatric floors; custody disputes may spill over into the hospital.
Policies on how to deal with estranged parents should be in place, as well as procedures for proving that abuse-protection and custody orders are valid. For more information on security measures used to prevent babies from being improperly removed from the hospital, see Preventing Infant Abductions.
Parking lots and other exterior areas. Several factors can contribute to a parking area becoming the scene of violence. Parking areas may be dark, may offer many hiding places, and may be deserted at certain hours.
Home care. Home care workers, who often must enter patients homes alone, are particularly vulnerable to violence. Home care workers may be exposed to unsafe conditions and have reported feeling threatened when they know that loaded weapons are present in a patients home, or that drive-by shootings or gang violence have occurred in the neighborhood. Rats, other vermin, or hostile animals may be present, or housing may be in a deteriorated condition, or other situations may exist that suggest the potential for physical violence, verbal abuse, or sexual harassment by patients, family members, or visitors (Gershon et al.). For more information on risks and strategies for home care workers, see the guidance articles Home Care: An Overview and Home Care: Staff-Related Risks, and the self-assessment questionnaires Home Care: Management and Operations and Home Care: Staff-Related Risks.
Types of Workplace Violence
The Federal Bureau of Investigation (FBI) classifies workplace violence according to perpetrators, as follows (FBI Violence):
- Type 1: Violence perpetrated by criminals who have no connection with the workplace (e.g., thieves)
- Type 2: Violence perpetrated by those whom an organization serves (e.g., patients, families, visitors)
- Type 3: Violence perpetrated against coworkers, supervisors, or managers by a present or former employee
- Type 4: Violence perpetrated by someone who has a personal relationship with an employee (e.g., an abusive spouse)
Type 1 violence accounts for only a small number of healthcare workplace violence incidents. Type 2 violence is the most common cause of physical violence in the healthcare setting, and type 3 violence is the most prevalent type of healthcare workplace violence. (Wax et al.)
A violence reduction project conducted at a large American hospital found that 64% of incidents against healthcare workers were perpetrated by patients or their visitors (type 2), while 35% were perpetrated by coworkers (type 3). Additionally, researchers identified surgery as the sole clinical area in which incidents perpetrated by coworkers (type 3) outnumbered incidents perpetrated by patients (type 2) (Arnetz et al. Application).
Although the prevalence of type 4 workplace violence specific to healthcare is unknown, such incidents do occur. Moreover, the frequency of domestic violence perpetrated against women, in combination with the typically large proportion of female workers in healthcare organizations, creates the potential for serious events. (Sawyer)
Incident Types
?Healthcare workers may experience a range of violent acts. To understand the experiences of hospital nurses who responded to a validated electronic survey regarding violence perpetrated by visitors, see Table 1. Type of Violence Perpetrated by Visitors?.
????Table 1. Type of Violence Perpetrated by Visitors? ? |
|
|---|---|
| Type of Vio?lenc?e Perpetrated by Visitors? | Percentage of Nurses Experienced? |
| Verbal abuse? | 32.9%? |
| Shouting or yelling? | 35.8%? |
| Swearing or cursing? | 24.9%? |
| Physical abuse? | 3.5%? |
| Grabbing? | 1.1%? |
| Scratching or kicking? | 0.8%? |
| ?Source: Speroni KG, Fitch T, Dawson E, Dugan L, Atherton M. Incidence and cost of nurse workplace violence perpetrated by hospital patients or patient visitors?. J Emerg Nurs 2014 May;40(3):218-28.? | |
?
Worker Safety?
The potential impact of workplace violence on healthcare workersboth victims and witnessesis significant in both the short and long term. In addition to the most immediate consequences of psychological trauma, physical injury, or even death, affected healthcare workers report feelings of anger, shock, hurt, frustration, embarrassment, humiliation, and depression. (Wax et al.) A literature review on workplace violence in healthcare identified the following responses, likely to impact quality of care, for affected workers (Phillips):
- Increase in missed workdays
- Burnout
- Job dissatisfaction
- Decreased productivity
- Decreased sense of safety
- Increased self-protection with personal weapons (e.g., knives, firearms)
Patient Safety
Violence in the healthcare workplace, by its very nature, can put both patients and healthcare workers at risk. This may happen overtly, such as when a patient and a nurses aide were shot and killed for no apparent reason by an armed man at a Florida hospital in 2016 (HCPro).
Impact on patients can also be more subtle; violence in healthcare settings has many potential downstream effects. For example, a negative relationship has been reported between violence experienced by healthcare workers and patient-perceived quality of care (Arnetz and Arnetz). Additionally, worker-to-worker incivility in the operating department has been linked to a poorer safety climate and decreased compliance with recommended practices in the surgical environment (Hamblin et al. Catalysts).
Danger in the Absence of Physical Aggression
Regardless of whether physical aggression is involved, verbal threats are associated with independent risk for workplace violence. Verbal assault is a risk factor for battery and future serious incidents of violence (Phillips; Schnapp et al.). Research also shows a significant relationship between hospital workers who were subject to verbal assault by a colleague and the risk of work-related injuries (Hamblin et al. Catalysts).
Costs
Loss of life, injury, and suffering by patients and healthcare workers alike are obvious costs of violence in healthcareand the financial implications are significant. OSHA reports that just one serious injury can result in workers compensation losses of thousands of dollars, in addition to thousands more for overtime, temporary staffing, or recruiting and training a replacement. (OSHA Prevention) The overall cost associated with workplace violence to all American businessesnot exclusively healthcareis an estimated $120 billion a year (Papa and Venella).
Potential hidden costs that organizations may incur include those for counseling affected individuals, the time required for managers and administrators to handle the issue and participate in the investigation, and increased medical claims for stress-related conditions. The publicity that follows a violent act in a healthcare setting can also do long-term damage to an organizations reputation. (Papa and Venella) Other hidden costs include increased worker turnover and decreased productivity and morale (OSHA Prevention).
Workers Compensation
In a retrospective database review of violence perpetrated against nurses by patients or visitors in a U.S. urban and community hospital system, annual costs for the 2.1% of nurses reporting workplace violence injuries were $94,156, including $78,924 for treatment and $15,232 for indemnity (Speroni et al.).
Lawsuits
Litigation that follows acts of workplace violence is a major direct cost. The average jury award in workplace violence cases in which an employer failed to take proactive, preventive measures has been reported as $3.1 million per person per incident. (Papa and Venella)
Three police officers employed by a Michigan hospital sued the owner of the parent medical system for $1 million each in 2016, alleging that they faced retaliation in response to filing complaints about crime and violence on the hospital campus. One of the officers reportedly questioned, Hospitals are supposed to be safe havens. If we, as the first line of defense, arent safe, how are we going to keep patients and their visitors safe? (Kurth)
?REGULATIONS AND STANDARDS
Federal Law
The general-duty clause of the Occupational Safety and Health Act (OSH Act) broadly addresses a multitude of workplace safety issues by requiring employers to furnish employees with employment and with a place of employment free from recognized hazards that cause or are likely to cause death or serious physical harm (29 USC § 654[a][1-2]).
Courts have interpreted the general-duty clause to mean that an employer has a legal obligation to provide a workplace free of conditions or activitiesfor example, workplace violencethat either the employer or industry recognizes as hazardous and that cause, or are likely to cause, death or serious physical harm to employees when there is a feasible method to abate the hazard. OSHA can cite and fine employers who fail to take reasonable steps to prevent or abate a recognized violence hazard in the workplace. (OSHA Fact Sheet)
OSHA Guidance
In 2016, OSHA released updated guidance on preventing violence in healthcare and social service settings. The guidance is advisory in nature; it is not a standard or regulation, and it does not create new legal obligations or alter existing obligations created by OSHA standards or the OSH Act. (OSHA Guidelines) However, it does provide a wealth of practical strategies for violence prevention.
There have been signals that OSHAs protection of the healthcare workforce may become increasingly robust. For example, in a 2016 report, GAO recommended that OSHA increase its education and enforcement efforts; OSHA agreed and stated that it would take action to address the following steps (GAO):
- Provision of additional information for inspectors on developing citations
- Follow-up on hazard alert letters
- Assessment of efforts to address workplace violence in healthcare settings to determine whether additional action is needed
Furthermore, OSHA is also considering the need for a specific standard to protect healthcare workers from workplace violence. In 2016, the agency published a request for information in the Federal Register, seeking public comments on the extent and nature of workplace violence in the healthcare industry as well as the nature and effectiveness of interventions and controls for violence prevention. (OSHA Prevention) The American Hospital Association has argued against the need for such a standard (American Hospital Association).
OSHA Reporting and Record-Keeping
?ECRI RESOURCES
|
|---|
Violent events that result in worker or staff injuries requiring treatment beyond first aid or requiring days away from work must be reported to OSHA, per agency standard (29 CFR § 1904). Employers must record these injuries in the OSHA Form 300 Log of Work-Related Injuries and Illnesses. Employers must report all work-related fatalities within 8 hours of learning of them, and must report the following occurrences within 24 hours of learning of them (OSHA Updates):
- All work-related inpatient hospitalizations of one or more employees
- All work-related amputations
- All work-related losses of an eye
For more information on OSHAs record-keeping standard and injury reporting forms, see OSHA Illness and Injury Record-Keeping Standard.
OSHA Inspections
OSHA may conduct an inspection in response to complaints or reports of workplace violence. According to Joint Commission, the agency typically evaluates the need for an inspection according to the following factors (Joint Commission OSHA):
- Involvement of a known risk factor
- Evidenceor lack thereofthat the organization recognizes the potential for workplace violence
- Potential methods to address the hazards that lead to violence
For example, OSHA is more likely to inspect following a violent incident involving a known risk factor if previous incidents have occurred and potential methods existed to alleviate the risk factors (e.g., an attack on a nurse by a patients family member who has a history of violence toward staff), as opposed to following a random act of violence. (Joint Commission OSHA)
Federal Fines
Healthcare organizations that fail to properly protect employees from the dangers of workplace violence face the threat of being fined by OSHA. For example, a Pennsylvania home care provider in 2016 was fined nearly $100,000 after a home care worker was sexually assaulted. The agency found that the organization failed to provide an effective workplace violence prevention program even in the face of numerous reports of verbal, physical, and sexual assaults on employees. (OSHA Federal Inspectors)
In 2014, OSHA fined a New York hospital $70,000 for willful failure to protect employees from assaults by patients and visitors, substantiated by 40 incidents of violence by patients and visitors in a three-month period. Given that many employees were unaware of its existence or purpose, OSHA found the organizations workplace violence prevention program ineffective. (OSHA Brookdale)
State Law
State law may provide additional protection for healthcare workers. Some states including Maine, Connecticut, New York, New Jersey, Maryland, Illinois, Washington, Oregon, and Californiahave enacted laws that require employers to establish comprehensive workplace violence prevention programs for healthcare employees. Others have increased penalties for those convicted of assaulting a nurse or, in some cases, other healthcare workers. The laws vary in scope and groups of individuals protected. (OSHA Workplace Violence Prevention)
Such laws have proven effective in lowering injury rates and workers compensation costs. For example, in Washington State, a 28% decrease in the rate of workers compensation claims in the healthcare and social assistance industry occurred after a state rule took effect requiring hazard assessments, training, and incident tracking for workplace violence. (OSHA Workplace Violence Prevention)
State Fines
State regulators may levy fines for failure to protect employees from workplace violence. For example, in 2016, investigators identified 116 injuries related to patient and visitor violence at a Detroit hospital between 2012 and 2015 (Kurth). The Michigan Occupational Safety and Health Administration imposed a $5,000 fine and required implementation of a plan to address routine exposure of healthcare and security employees to violent behavior by patients and visitors (Rege).
Joint Commission
The following Joint Commission standards address workplace violence in accredited healthcare settings (Joint Commission Comprehensive):
- Standard LD.03.01.01 requires leaders to create and maintain a culture of safety and quality throughout the organization, which impacts both patient and worker safety
- Standard LD.04.04.05 requires an organization-wide safety program, and requires systems for blame-free incident reporting
- Standard EC.02.01.01 requires organizations to manage safety and security risks
- Standard EM.02.02.05 requires organizations to maintain emergency operations plans describing how the facility will coordinate security activities with community security agencies
Additionally, Joint Commission considers the rape, assault (leading to death or permanent loss of function), or homicide of a staff member, licensed independent practitioner, visitor, or vendor while on site at the health care organization to be a sentinel event (Joint Commission Sentinel).
DNV
Det Norske Veritas Germanischer Lloyd (DNV-GL) quality management standards require accredited hospitals to maintain safe and secure facilities that are designed and maintained in accordance with national and local laws, hospital policy, regulations and guidelines. Standards further specify that the Security Management System shall address issues related to abduction, elopement, visitors, workplace violence, and investigation of property losses and [shall] be proportional to the risk. (DNV-GL, PE 4, SR 3)
Professional Associations
Professional associations including the American College of Emergency Physicians, the American Nurses Association, and the Emergency Nurses Association have issued policies, position statements, and resources regarding workplace violence. See Resource List? for more information.
?ACTION PLAN
Establish?Policies and Procedures
Action Recommendation: Develop and enforce comprehensive policies and procedures against workplace violence.
?Organizations should develop and enforce comprehensive policies and procedures, such as the following, against violence perpetrated by visitors, staff, patients, or other individuals. All policies concerning violent events should be applied consistently to all individuals. ?
Zero tolerance. A zero-tolerance policy, which states that any form of violence is not acceptable, applies to all employees, patients, and visitors (ACEP Protection). Although zero tolerance does not mean that violence will not happen, it sets the expectation that violence will not be tolerated and will be dealt with according to policy. Such a policy should explicitly acknowledge verbal assault as a form of violence, because tolerance of verbal abuse and low-level battery invites more serious forms of violence (Phillips). The policy should also specify actions that are grounds for termination or discipline (e.g., committing an act of violence, failing to report an act of violence) (Hamer).
Mandatory reporting. A mandatory reporting policy requires all staff to report any actual or threatened physical or verbal assault without delay (ACEP Protection).
Nonretaliation. A nonretaliation policy should explicitly forbid any adverse employment action (e.g., actual or threatened termination, demotion, suspension, discrimination) against an employee for good-faith reporting of actual or threatened violence (ACEP Protection).
Response to violence. Procedures for responding to incidents of workplace violence should clearly address designated employee roles and responsibilities for notifying managers and security, activating emergency response codes, and incident reportin
